Have you noticed of late a gradual increase of stiffness and/or pain in your shoulder, sometimes without any obvious mechanism of injury? Wondering why on earth lying on one side of your body at night is agony, and basic tasks like getting dressed or hanging the washing on the line are getting harder and harder?
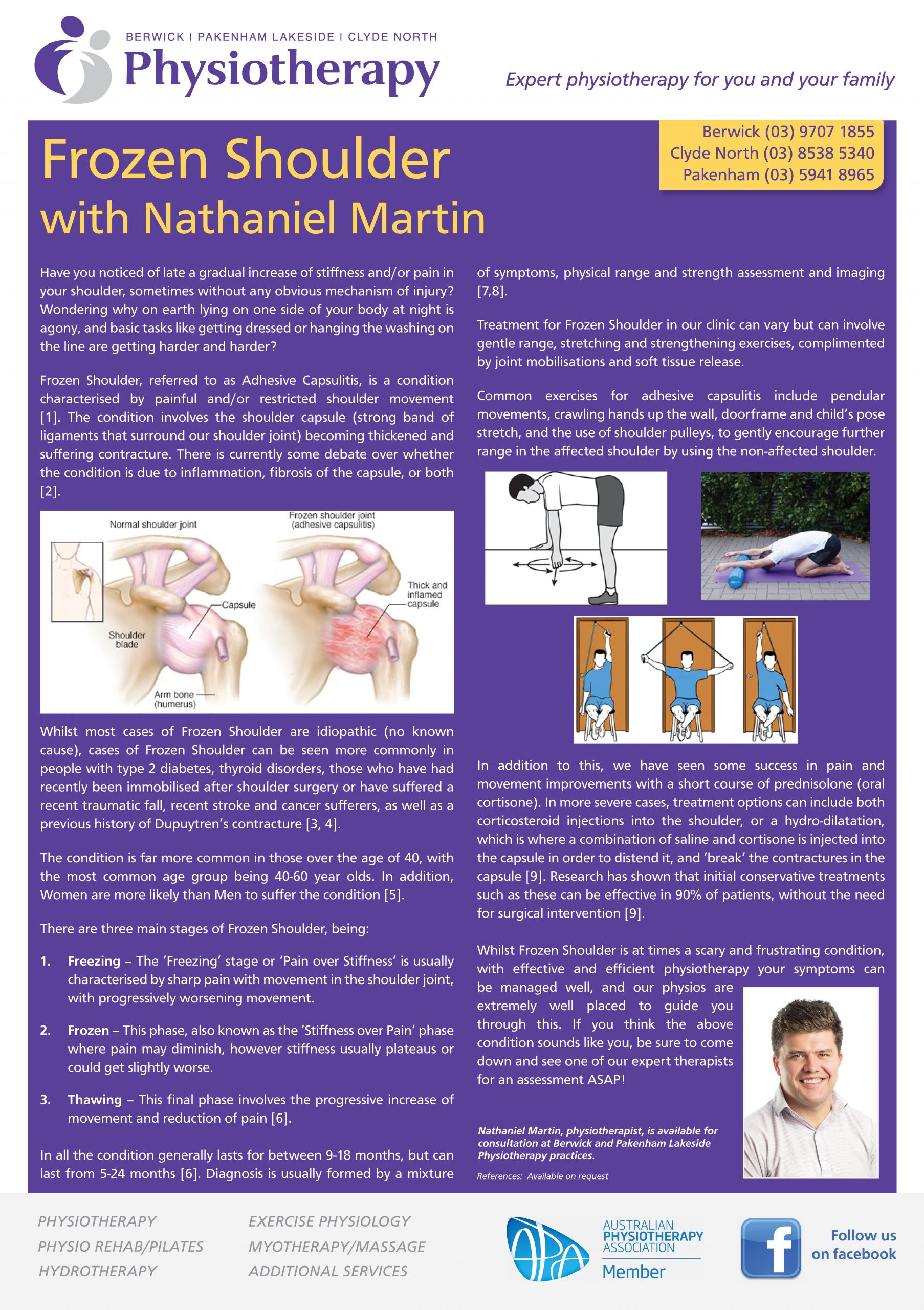
Frozen Shoulder, referred to as Adhesive Capsulitis, is a condition characterised by painful and/or restricted shoulder movement [1]. The condition involves the shoulder capsule (strong band of ligaments that surround our shoulder joint) becoming thickened and suffering contracture. There is currently some debate over whether the condition is due to inflammation, fibrosis of the capsule, or both [2].
Whilst most cases of Frozen Shoulder are idiopathic (no known cause), cases of Frozen Shoulder can be seen more commonly in people with type 2 diabetes, thyroid disorders, those who have had recently been immobilised after shoulder surgery or have suffered a recent traumatic fall, recent stroke and cancer sufferers, as well as a previous history of Dupuytren’s contracture [3, 4].
The condition is far more common in those over the age of 40, with the most common age group being 40-60 year olds. In addition, Women are more likely than Men to suffer the condition [5].
There are three main stages of Frozen Shoulder, being:
- Freezing – The ‘Freezing’ stage or ‘Pain over Stiffness’ is usually characterised by sharp pain with movement in the shoulder joint, with progressively worsening movement.
- Frozen – This phase, also known as the ‘Stiffness over Pain’ phase where pain may diminish, however stiffness usually plateaus or could get slightly worse.
- Thawing – This final phase involves the progressive increase of movement and reduction of pain [6].
In all the condition generally lasts for between 9-18 months, but can last from 5-24 months [6]. Diagnosis is usually formed by a mixture of symptoms, physical range and strength assessment and imaging [7,8].
Treatment for Frozen Shoulder in our clinic can vary but can involve gentle range, stretching and strengthening exercises, complimented by joint mobilisations and soft tissue release.
Common exercises for adhesive capsulitis include pendular movements, crawling hands up the wall, doorframe and child’s pose stretch, and the use of shoulder pulleys, to gently encourage further range in the affected shoulder by using the non-affected shoulder.
In addition to this, we have seen some success in pain and movement improvements with a short course of prednisolone (oral cortisone). In more severe cases, treatment options can include both corticosteroid injections into the shoulder, or a hydro-dilatation, which is where a combination of saline and cortisone is injected into the capsule in order to distend it, and ‘break’ the contractures in the capsule [9]. Research has shown that initial conservative treatments such as these can be effective in 90% of patients, without the need for surgical intervention [9].
Whilst Frozen Shoulder is at times a scary and frustrating condition, with effective and efficient physiotherapy your symptoms can be managed well, and our physios are extremely well placed to guide you through this. If you think the above condition sounds like you, be sure to come down and see one of our expert therapists for an assessment ASAP!
References: [1] Dias R, Cutts S, Massoud S. Frozen shoulder. Bmj. 2005 Dec 15;331(7530):1453-6; [2] Cho CH, Song KS, Kim BS, Kim DH, Lho YM. Biological aspect of pathophysiology for frozen shoulder. BioMed research international. 2018 May 24;2018; [3] Mezian K, Chang KV. Frozen Shoulder. StatPearls [Internet]. 2019 Feb 25; [4] Whelton C, Peach CA. Review of diabetic frozen shoulder. European Journal of Orthopaedic Surgery & Traumatology. 2018 Apr;28(3):363-71; [5] Uppal HS, Evans JP, Smith C. Frozen shoulder: a systematic review of therapeutic options. World journal of orthopedics. 2015 Mar 18;6(2):263; [6] Chan HB, Pua PY, How CH. Physical therapy in the management of frozen shoulder. Singapore medical journal. 2017 Dec;58(12):685; [7] Kelley MJ, Shaffer MA, Kuhn JE, Michener LA, Seitz AL, Uhl TL, Godges JJ, McClure PW, Altman RD, Davenport T, Davies GJ. Shoulder pain and mobility deficits: adhesive capsulitis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the Orthopaedic Section of the American Physical Therapy Association. Journal of orthopaedic & sports physical therapy. 2013 May;43(5):A1-31; [8] Li JQ, Tang KL, Wang J, Li QY, Xu HT, Yang HF, Tan LW, Liu KJ, Zhang SX. MRI findings for frozen shoulder evaluation: is the thickness of the coracohumeral ligament a valuable diagnostic tool?. PLoS One. 2011 Dec 7;6(12):e28704; [9] Cho CH, Bae KC, Kim DH. Treatment strategy for frozen shoulder. Clinics in orthopedic surgery. 2019 Sep;11(3):249.