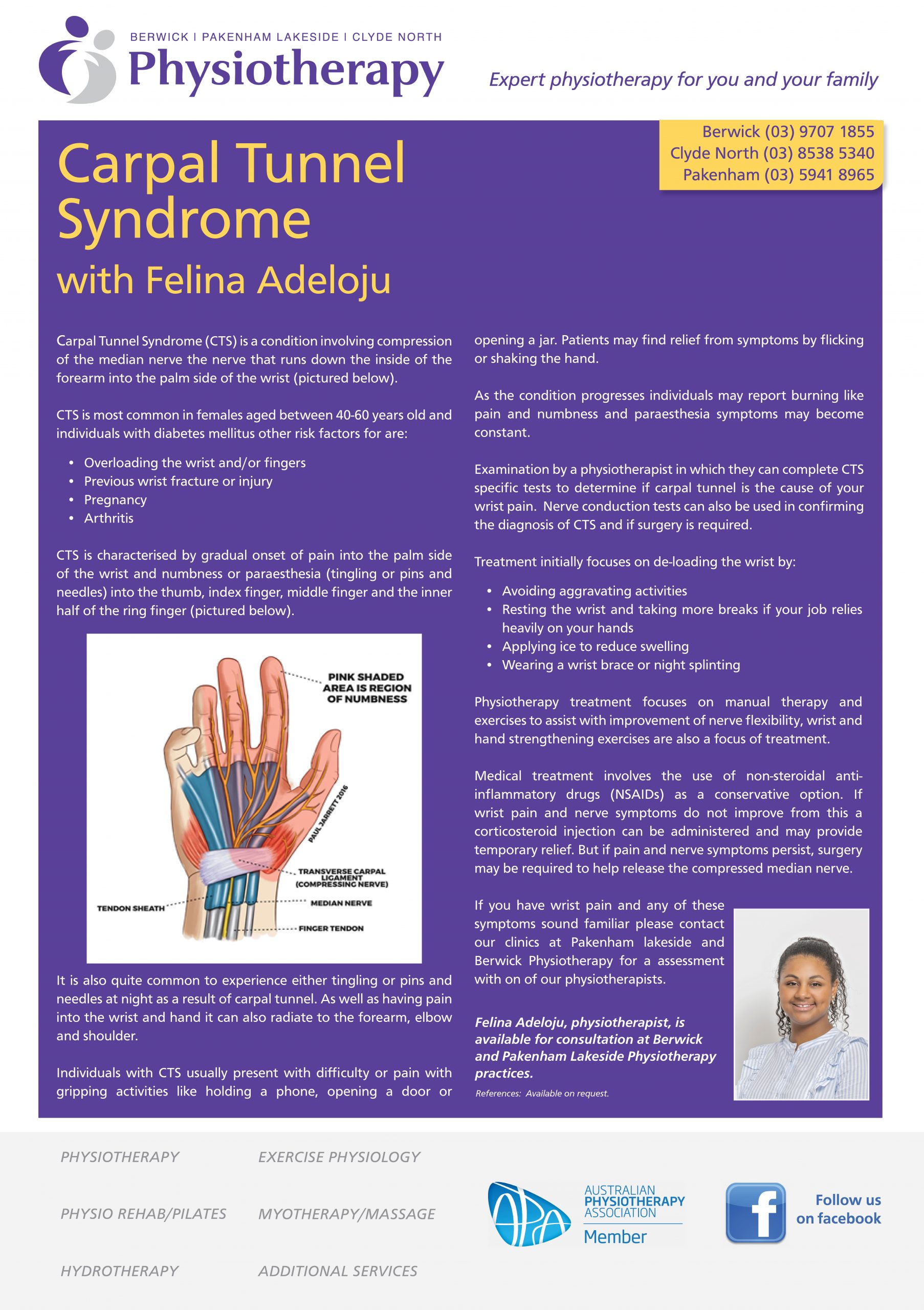
Carpal Tunnel Syndrome (CTS) is a condition involving compression of the median nerve the nerve that runs down the inside of the forearm into the palm side of the wrist (pictured below).
CTS is most common in females aged between 40-60 years old and individuals with diabetes mellitus other risk factors for are:
- Overloading the wrist and/or fingers
- Previous wrist fracture or injury
- Pregnancy
- Arthritis
CTS is characterised by gradual onset of pain into the palm side of the wrist and numbness or paraesthesia (tingling or pins and needles) into the thumb, index finger, middle finger and the inner half of the ring finger (pictured below).
It is also quite common to experience either tingling or pins and needles at night as a result of carpal tunnel. As well as having pain into the wrist and hand it can also radiate to the forearm, elbow and shoulder.
Individuals with CTS usually present with difficulty or pain with gripping activities like holding a phone, opening a door or opening a jar. Patients may find relief from symptoms by flicking or shaking the hand.
As the condition progresses individuals may report burning like pain and numbness and paraesthesia symptoms may become constant.
Examination by a physiotherapist in which they can complete CTS specific tests to determine if carpal tunnel is the cause of your wrist pain. Nerve conduction tests can also be used in confirming the diagnosis of CTS and if surgery is required.
Treatment initially focuses on de-loading the wrist by:
- Avoiding aggravating activities
- Resting the wrist and taking more breaks if your job relies heavily on your hands
- Applying ice to reduce swelling
- Wearing a wrist brace or night splinting
Physiotherapy treatment focuses on manual therapy and exercises to assist with improvement of nerve flexibility, wrist and hand strengthening exercises are also a focus of treatment.
Medical treatment involves the use of non-steroidal anti-inflammatory drugs (NSAIDs) as a conservative option. If wrist pain and nerve symptoms do not improve from this a corticosteroid injection can be administered and may provide temporary relief. But if pain and nerve symptoms persist, surgery may be required to help release the compressed median nerve.
If you have wrist pain and any of these symptoms sound familiar please contact our clinics at Pakenham lakeside and Berwick Physiotherapy for a assessment with on of our physiotherapists.
References: Brukner, P. (2017). Brukner & Khan’s clinical sports medicine. (5th Edition) North Ryde: McGraw-Hill. Genova, A., Dix, O., Saefan, A., Thakur, M., & Hassan, A. (2020). Carpal tunnel syndrome: a review of literature. Cureus, 12(3). Chesterton, L. S., Blagojevic-Bucknall, M., Burton, C., Dziedzic, K. S., Davenport, G., Jowett, S. M., … & Roddy, E. (2018). The clinical and cost-effectiveness of corticosteroid injection versus night splints for carpal tunnel syndrome (INSTINCTS trial): an open-label, parallel group, randomised controlled trial. The Lancet, 392(10156), 1423-1433. Bobowik, P. Ż. (2019). Effectiveness of physiotherapy in carpal tunnel syndrome (CTS). Postępy Rehabilitacji, 2019(2), 47-58. doi:10.5114/areh.2019.8502